The Respiratory System
- Created by: rosieevie
- Created on: 20-01-17 17:11
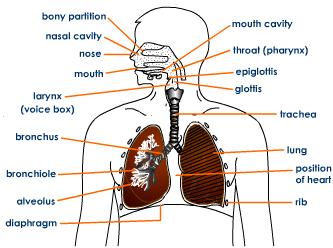
Structure of Respiratory System
Lung Compliance
- Relating to lung elasticity
- Decrease - sitffer lung = harder to infalte
- Increase - floppy lung = tissue collapse (especially on exhalation) - emphasema

Alveoli
- Air-filled sacs - expand during inhalation
- Covered with extensive vasculature - gasous exchange
- 3 cell types:
- Type I cell - simple squamous - flat and narrow = thin diffusion pathway
- Type II cell - produce surfactant = detergent which decreases surface tension
- Alveolar macrophages - white blood cell = defence (purify air/immune response)
- Alveolar surface tension - keeps alveolar open and prevents collapse into bigger structures due to pressure difference (surfactanct reduces and equalises pressure)
Spirometry Trace Labelled
- Volume - amount of space take up by an object
- Capacity - measure of object's ability to hold a substance
Blood Gaseous Exhange
Oxygen diffuses into blood along partial pressure gradient - changes caused by breathing and circulation.
Warm, humid air in lungs means lower pp in alveoli than atmospheric air
Dalton's Law - in a mixture of gases (air) the total pressure is sum of gas partial pressures
Partial pressure - the pressure a gas would exert if only gas present

At sea level (mostly N2 and O2) - Ptotal = 760mmHg
- N2 = 760mHg x 0.78 = 560mmHg
- O2 = 760mmHg x 0.21 = 160mmHg
Changing altitude = change oxygen's partial pressure
Diffusion Across a Membrane (Fick's Law)
Vgas = (AD/T) x (P1 - P2)
- Vgas = diffusion rate
- A = Area of pathway (directly proportional - large alveolus SA)
- D = gas solubility (directly proportional)
- Limiting factor - reduced by haemoglobin and carbonic anhydrase
- T = pathway thickness (inversly proportional - single squaemous epithelial layer)
- P1 and P2 = pressure differential (directly proportional - high diffusion gradient maintainined by ventilation and circulation)

Oxygen-Haemoglobin Dissociation Curve
Carbon Dioxide Transport
- Binds to globin protein of haemoglobin = carbamminoHb (20%
- Dissolves in blood plasma (10%)
- HCO3- in blood plasma (70%)
Carbon dioxide conversion to HCO3-:
RBC facilitate conversion using carbonic anhydrase enzyme:

RBC O2 carrying role not independent of CO2 carrying role = related reactions - removing H+ ions from O2 reaction drives CO2 reaction
Comments
No comments have yet been made